What are organ-on-chip models?
Organ-on-chip models are microfluidic systems that simulate the physiological microenvironment of human organs at the cellular level. They include living cells, dynamic flow conditions, and mechanical cues in order to replicate organ function. These systems fill the gap between conventional in vitro cell cultures and animal models by providing a controlled, biomimetic environment for studying human pathophysiology and drug responses.
What are the primary drawbacks of the use of animal models in drug testing?
There are some important limitations of animal models: they do not match humans in the anatomy of the lungs, cell morphology, and localization; they give an incomplete picture of the disease features; findings made are hard to compare across laboratories and among species; and they are hard to translate to clinical trials in humans. Also, animal testing is ethical but involves high costs in terms of money and time.
Why are conventional 2D cell cultures inadequate in drug testing?
Classical 2D cell cultures are systems that do not mimic the dynamic living tissue environment. They block different cell types in co-culture, cannot simulate the lung airway interface, and do not provide the mechanical stimuli present in the body. Although straightforward and applicable to some clinical diagnoses, such as tuberculosis testing, they provide little information about the complex organ-level responses.
What are the benefits of using organ-on-chip models as compared to ex vivo cultures?
Organ-on-chip models are long-term viable and reproducible compared to ex vivo cultures of biopsy samples. Ex vivo samples maintain normal tissue structure but their viability is limited with regard to time, the barrier properties are damaged by external factors, and cross-sample variability. These limitations are overcome using organ-on-chip systems based on controlled microenvironments.
What are the differences between organ-on-chip models and organoids?
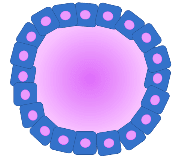
Although organoids offer a 3D microenvironment and have the potential to recap the organ formation, they lack immune and vascular components and have a low level of control of the stem cell behavior and reproducibility. Organ-on-chip models are used to solve these shortcomings by including blood vascular structures, creating a well-controlled cellular environment, and incorporating physiological parameters monitored in real-time with sensors.
What are the organ-on-chip systems fabrication benefits?
Organ-on-chip fabrication has provided modularity and multiple methods and materials, simple design development and alteration, high protocol reproducibility, and sensor integration possibilities to provide high-throughput judgments. Technology allows the creation of individual models that are specific to a single patient or the disease situation and thus will be highly applicable in research and drug development.
What is the advantage of the microscale flow in the organ-on-chip models?
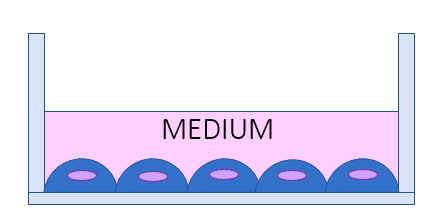
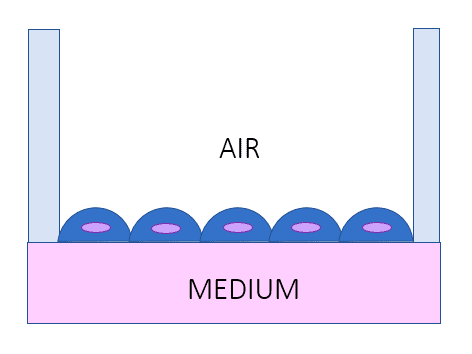
Microscale flow facilitates the ability of such systems to recapitulate physiological and disease mechanical cues on cellular and tissue scales. It produces controlled and dynamic micro environments which is a close replica of the in vivo environment such as the re-creation of important interfaces such as the air-liquid interface in the lung models. This dynamism is critical to proper modeling of organ response and drug reactions.
What cellular benefits are offered by organ-on-chip models?
These models produce complex tissue-like environments using many cell types, which can allow researchers to build modular devices to recapitulate different areas of an organ. In the case of lungs, it involves bronchi and alveoli areas. The systems are able to recreate the physiological and pathological conditions that offer insights that are more applicable in understanding the mechanisms of diseases and therapeutic intervention.
Which benefits in terms of cost and time does organ-on-chip models bring?
The organ-on-chip technology is used to quickly fabricate using soft lithography and quick prototyping technology. Researchers are able to test drugs and compounds on a high-throughput basis. The cost and time involved in developing the drug and testing an illness is greatly reduced by the capability to mimic the conditions of a disease with ease, avoid the preparation of animal models, their maintenance, and usage.
What are the weaknesses of tissue engineering techniques that the organ-on-chip models aim to solve?
Standard formulations of tissue engineering, which rely on artificial or decellularized scaffolds, have difficulties in recapitulating structural and mechanical forces or autonomous production of ECM. Organ-on-chip models address these drawbacks by offering the ability to control mechanical stimulation, dynamic micro-environment and integrating many tissue-based components to build more physiologically relevant systems more suited to drug testing and disease modeling.